|
||||||||||||
|
||||||||||||
 |
||||||||||||
|
||||||||||||
The Newborn Instrument Production Project was established by Kriangsak Jirapaet, MD, Professor Emeritus of Pediatrics (Neonatology), in 1984 with the support of the Faculty of Medicine Siriraj Hospital, Mahidol University. |
||||||||||||
Vision and mission |
||||||||||||
|
||||||||||||
Research and development |
||||||||||||
|
||||||||||||
 |
||||||||||||
The aim of production |
||||||||||||
The Siriraj phototherapy device (SPD) was first produced in 1996 using fluorescent tubes to solve the high rate of blood exchange transfusions from hyperbilirubinemia at Siriraj Hospital, approximately 500 cases per year. The Siriraj phototherapy device has evolved significantly through continuous improvement, from daylight fluorescent tubes to special blue fluorescent tubes,1-4 and advanced to light-emitting diode (LED) tubes as a light source for intensive phototherapy. The advantage of SPD is that the traditional SPD using fluorescent tubes can be easily modified to use LED tubes by simply adding an LED conversion kit and replacing the fluorescent tubes with LED tubes, which helps the hospital save on the budget for purchasing a new LED phototherapy device. In addition, its T8-LED tube enclosure can also support the future development of LED tubes when compared to phototherapy machines using LED modules that may not be able to. |
||||||||||||
|
||||||||||||
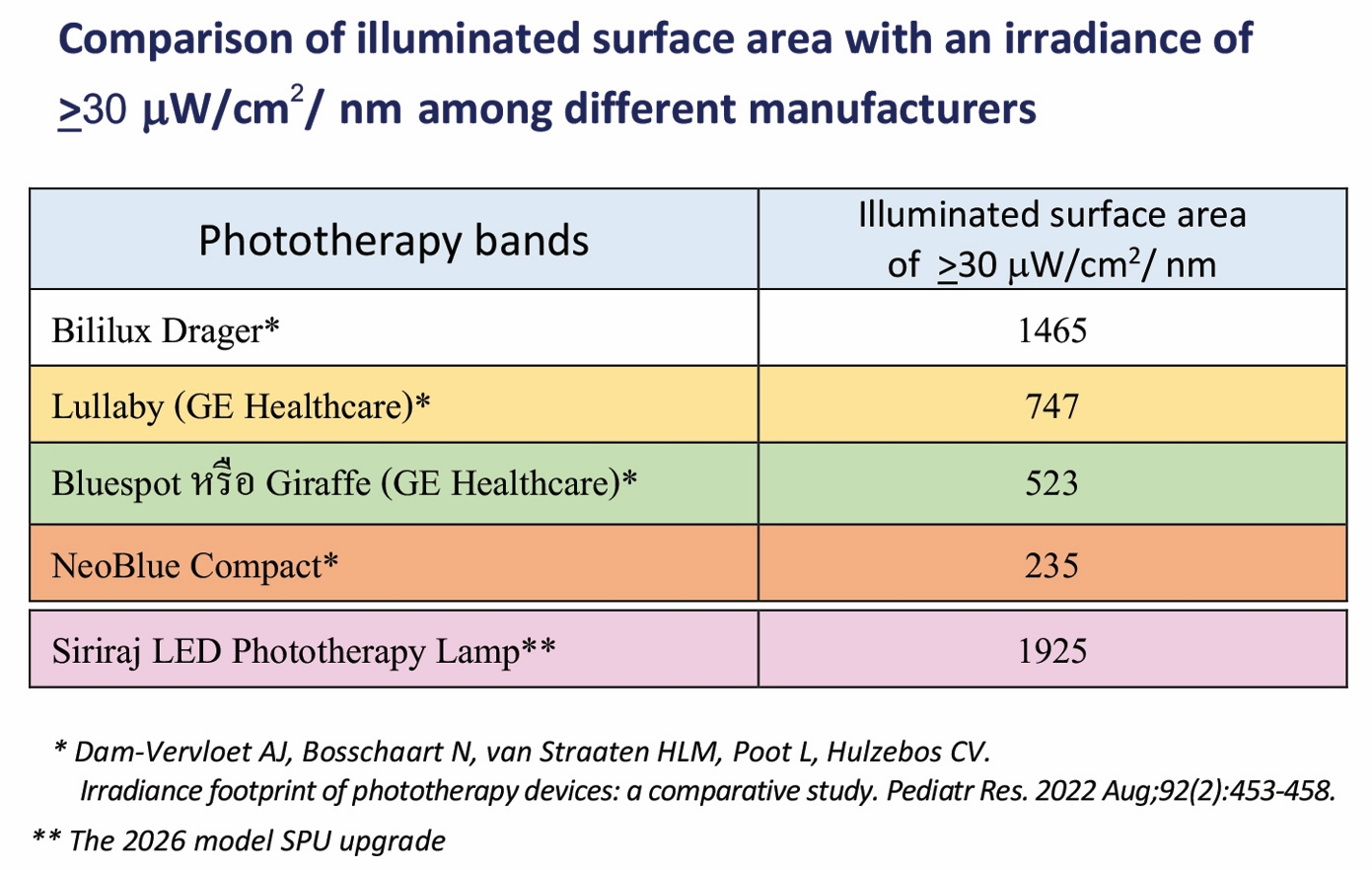
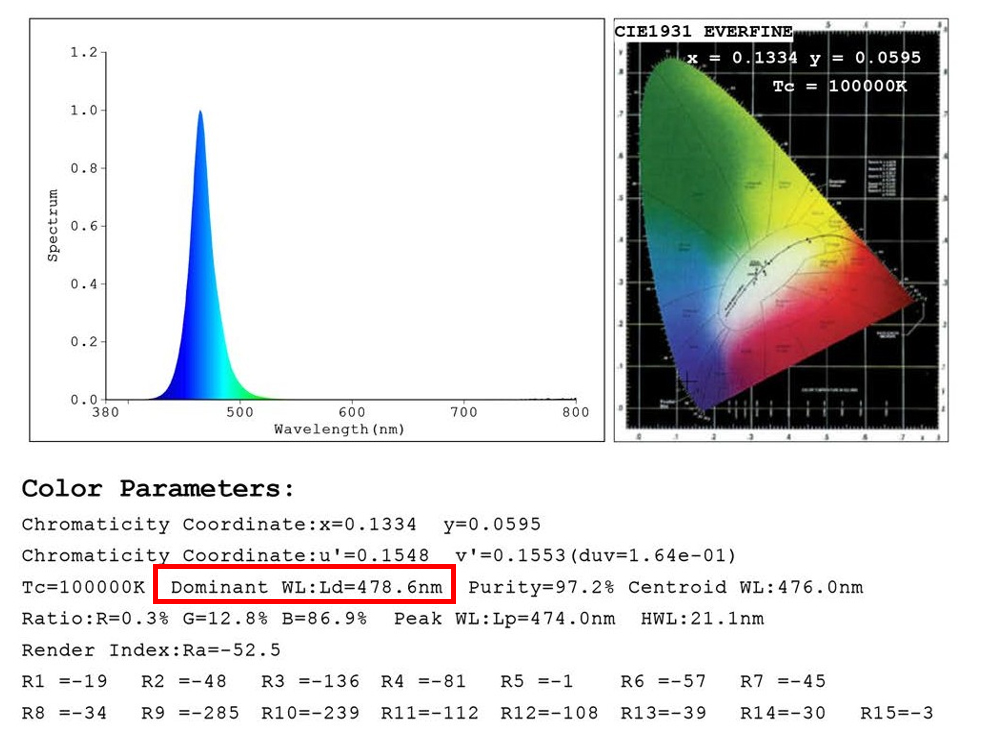
| The latest SPD design has been upgraded to be modern for LED phototherapy for neonatal jaundice. The latest SPD design aligns with the American Academy of Pediatrics (AAP) recommendations for the most effective and safe phototherapy devices.5 These include: (1) incorporation of narrow band blue-to-green light-emitting diode lamps (∼460–490 nm wavelength range; 478 nm optimal), (2) emission of irradiance of at least 30 µW/cm2/nm in term infants, and (3) illumination of the exposed maximal body surface area of an infant (100%). The key improve-ment is using the blue-green wavelength of a peak ~478 nm, which has previously shown 31% more efficient for removing unconjugated bilirubin from circulation than blue LED light with a peak wavelength of ~452 nm6. This wavelength increases the safety profile by reducing photodynamic damage, minimizing heat generation, and limiting oxidative stress.6,7 | ||||||||||||
|
||||||||||||
SPD is a floor-standing, mobile phototherapy device utilizing T8-LED tubes instead of integrated LED light modules. It offers significant advantages regarding maintenance costs and ease of repair. Users can replace the LED tubes themselves, and only the deteriorating tube needs to be replaced, rather than the complete integrated LED fixtures. |
||||||||||||
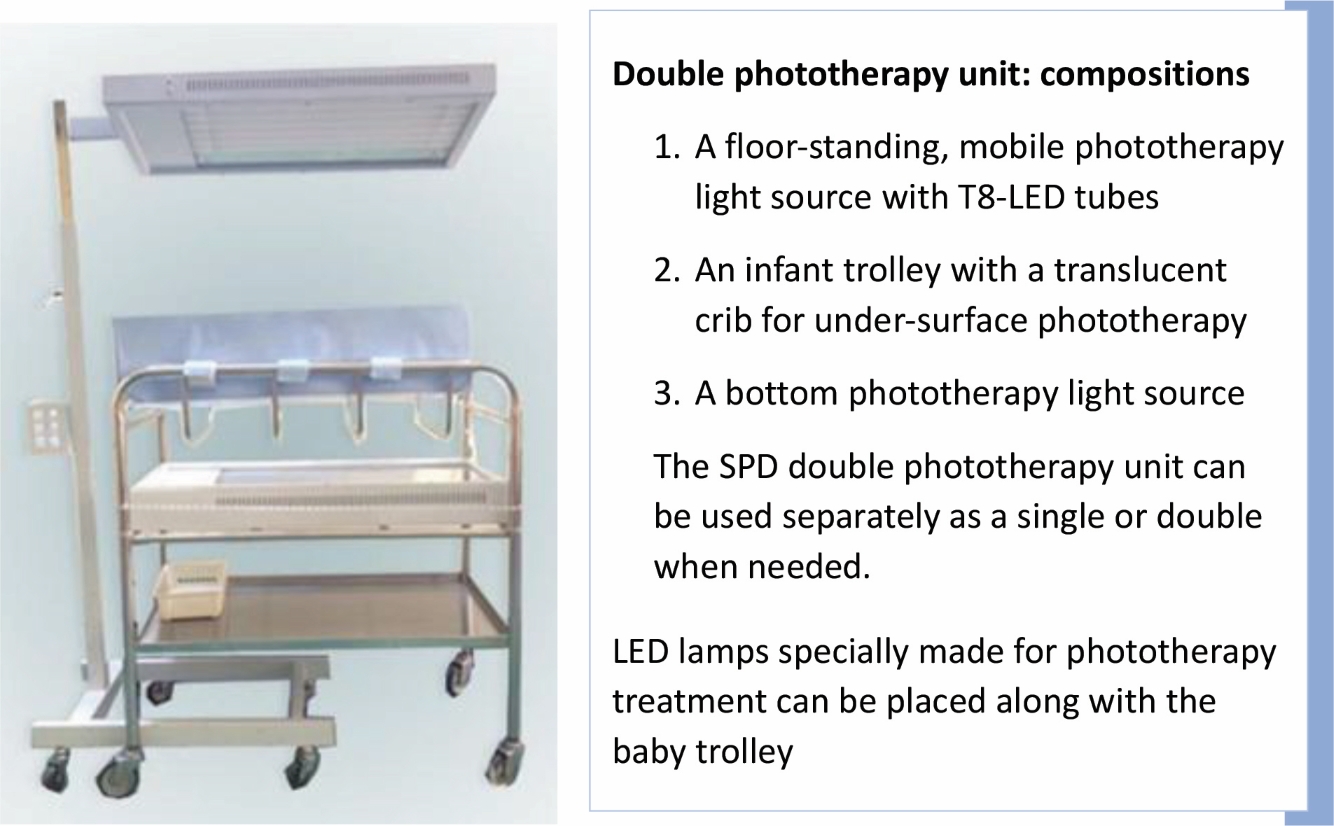
SPD provides high spectral irradiance that covers more than the entire body surface area of a full-term, 40-week gestational-age infant (1,925 cm2 vs 1,500 cm2). The distance of the light enclosure can be adjusted as needed to reduce or increase the irradiance intensity; a closer proximity to the baby increases the intensity. |
||||||||||||
|
||||||||||||
The LED tubes of SPD do not emit significant light in the ultraviolet or infrared ranges, with a reduced risk of skin damage and a minimal increase in the air temperature surrounding the baby from the thermal energy dissipated into the surrounding air by the LED heat sink. |
||||||||||||
|
||||||||||||
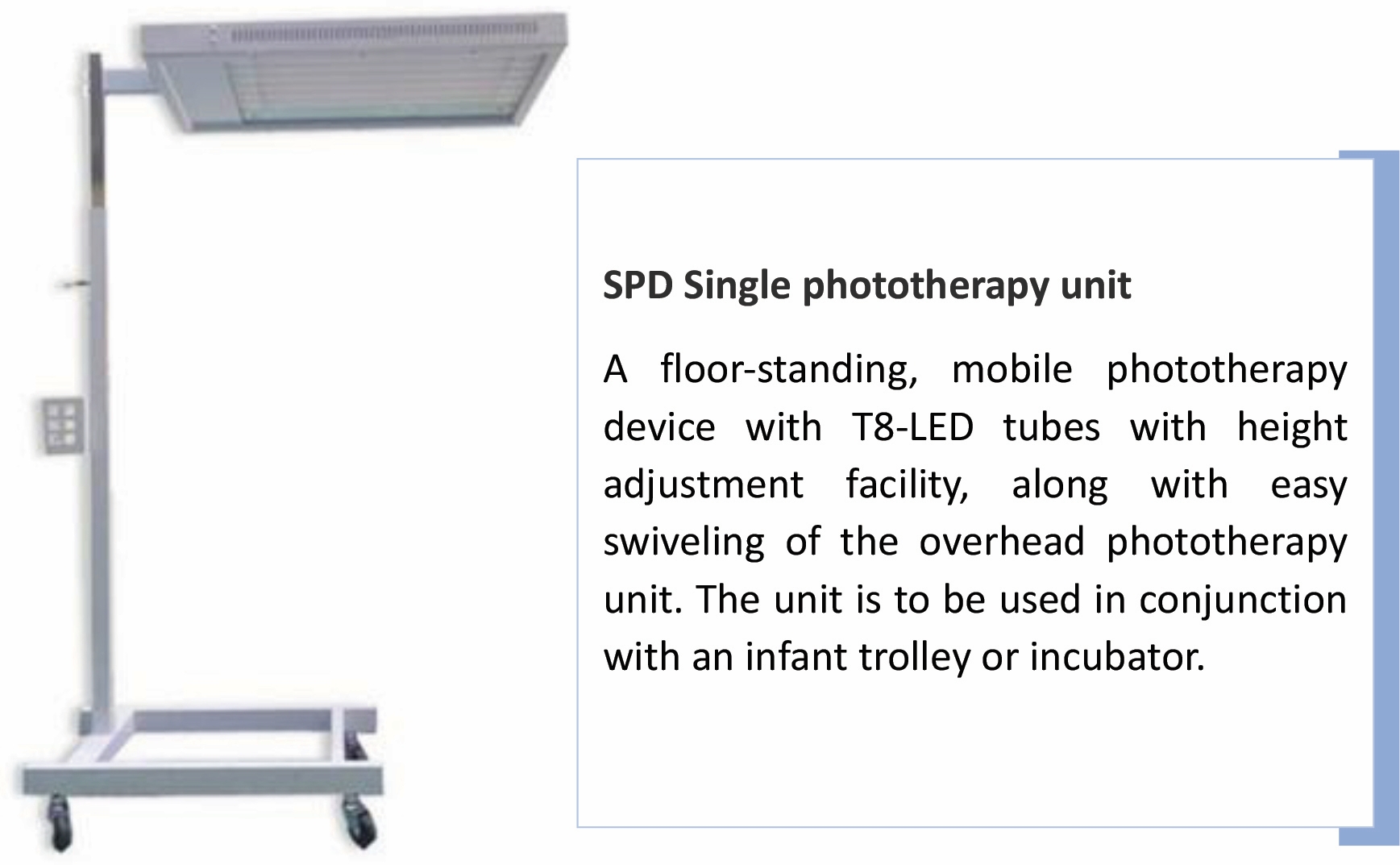
| SPD is available in both single and double phototherapy units. | ||||||||||||
Product specification |
||||||||||||
 |
||||||||||||
 |
||||||||||||
 |
||||||||||||
 |
||||||||||||
Spectrum |
||||||||||||
| This SPD upgrade utilizes blue–green LED light with a peak emission of 478 nm, which has proven 31% more effective in removing unconjugated bilirubin from circulation than blue LED light with a peak wavelength of 452 nm.6 | ||||||||||||
 |
||||||||||||
Intensity |
||||||||||||
| The use of six T8-LED tubes provides more light energy and uniform distributions of light energy. SPD emits a light energy of 66.8 microwatts/cm2/nm in the center of the ISA, covering the head to toes, with an average light energy of 49.5 μW/cm2/nm calculated from an ISA for 40-week-gestational-term infants of 30x50 cm (the blue-green area). | ||||||||||||
The effectiveness of SPD for treating jaundice |
||||||||||||
| Compared to the daylight fluorescent phototherapy device and the foreign LED device, the first SPD invented with special blue fluorescent tubes showed a faster bilirubin decrease in healthy infants (p-value < 0.015).2,4 The rate of blood transfusions reduced by 75% within the first 6 months of use, from 15.4% to 4.3%.2 The annual prevalence of exchange transfusions, which pose a risk to blood-transmitted diseases such as CMV, HIV, hepatitis B, C, etc., dropped to 19 cases per year after the double SPD was produced in 2003. | ||||||||||||
References: |
||||||||||||
1. Jirapaet K, Jirapaet V. Measurements of the irradiance and the effect on environment temperature of the Siriraj Phototherapy Lamp. Siriraj Hospital Gazette, 1997:49:323-9. |
||||||||||||
|
||||||||||||
The Newborn Instrument Production Project was established by Kriangsak Jirapaet, MD, Professor Emeritus of Pediatrics (Neonatology), in 1984 with the support of the Faculty of Medicine Siriraj Hospital, Mahidol University. |
||||||||||||
| Vision and mission |
||||||||||||
His vision has been that improving national neonatal care standards requires the ability to rely on inexpensive, independently produced, long-lasting, and high-quality medical equipment with low-cost maintenance. The project addresses the shortage of medical equipment needed for the care of newborn infants in Thailand. It is a significant barrier to addressing the public health issues that contribute to high neonatal morbidity and mortality. The project has been carried out since 1995 without support from Siriraj Hospital but with the same policy, and the equipment has been either sold to hospitals or donated to those with a limited budget to support the improvement of neonatal care standards on a nationwide level. |
||||||||||||
Research and development |
||||||||||||
All project medical devices have been researched and proven for their effectiveness, safety, and durability. Selling with less profit so the health service system can leverage their buying power for these vital medical devices. The device has been sold to hospitals across the country at a price that is 4-5 times cheaper than those imported from abroad. |
||||||||||||
 |
||||||||||||
The aim of production |
||||||||||||
SRW was first produced in 1986 to tackle the problem of neonatal hypothermia in the delivery room (DR) and neonatal wards due to a lack of infant warming devices (infant warmer, infant incubator, etc.). The prevalence of hypothermia was 52% for infants transferred from the DR to the well newborn nursery for 24-hour observation and 100% for those transferred to the sick newborn wards for treatment.1 It was intended as a simple and easy-to-use therapy warmer that provides warmth for preterm and term infants. SRW was awarded the Mahidol University Award for Invention by His Majesty King Bhumibol in 1991. It was one of the major achievements listed in the 120 Memorabilia of Siriraj book published in 2003 when the Faculty of Medicine Siriraj Hospital commemorated its 120-year anniversary.2 |
||||||||||||
General product information |
||||||||||||
The SRW is a floor-standing and moveable warmer and has been designed to be used with infants lying in open beds or with babies in incubators who need to open the cabinet for procedures (the concept design of a hybrid incubator nowadays). |
||||||||||||
 |
||||||||||||
Heating element |
||||||||||||
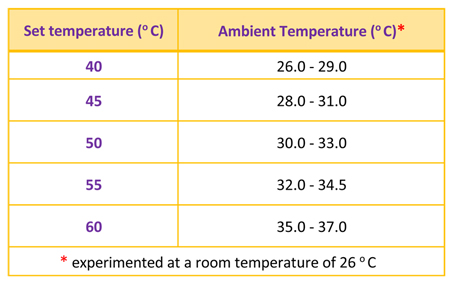
The enclosure, with a 1000-wat heater rod inside, can provide even heat distribution over the entire bed area. It is made of stainless steel and is located on a pole with a caster base, which makes it easy to move the device. The base can be inserted under the open bed and an incubator. The ambient temperature around an infant can be adjusted by setting the thermostat button in accordance with the required neutral thermal environment (NTE) temperature appropriate to its birthweight and age. NTE is an environment in which an infant maintains a normal body temperature while minimizing energy expenditure and oxygen consumption. Following is the relationship between the set temperature and ambient temperature when the lower edge of the enclosure is 90 cm above the infant and drafts are avoided. |
||||||||||||
 |
||||||||||||
The efficiency of SRW on Infants� temperatures |
||||||||||||
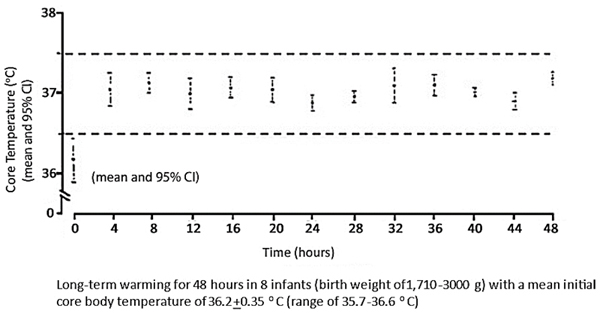
| Long-term temperature maintenance |
||||||||||||
The SRW has the capability to operate continuously. By using an adjustable thermostat in conjunction with a thermocouple, the device can be switched on and off intermittently. It can be used as a substitute for an incubator for preterm and term infants if one is lacking. But it must be free from drafts in the room environment to prevent hypothermia.1 The core temperatures can be maintained within the normal range of 36.5 °C to 37.5 °C.1 |
||||||||||||
 |
||||||||||||
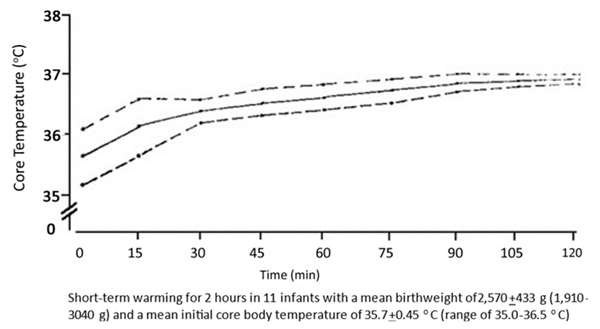
Short-term warming |
||||||||||||
SRW can effectively treat hypothermia in preterm and term infants within two hours of warming.1 |
||||||||||||
 |
||||||||||||
References: |
||||||||||||
|
||||||||||||
|
||||||||||||
|
||||||||||||